

Aortic stenosis
Author Ольга Кияница
2018-03-23
Stenosis of the aorta (CA) is a narrowing of the hole, which is located on the sort of aorta due to the connection of the valves of the valve. Such a violation is an obstacle to blood flow, resulting in the development of pathological changes in the left ventricle, in the severe cases - left ventricular insufficiency.
The first description of aortic stenosis was presented in 1663 by the French physician Lazar Rivier.
Aortic stenosis occurs for several reasons, including congenital anomalies of development, valvular calcination and acute rheumatic fever. Instrumental methods of investigation are important for the diagnosis of narrowing of the mouth of the aorta. Today, two-dimensional (2D) Doppler echocardiography is most commonly used today. For treatment, both medical and surgical effects are used.
Video: Aortic stenosis - "Just about the complex"
Description
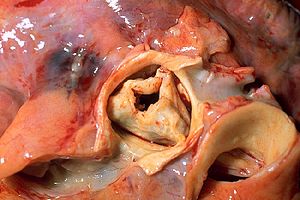
The aortic valve (in val.aortae) is located between the left ventricle (LV) and the mouth of the largest vessel, the aorta, which allows the blood to flow in only one direction. The basis of the valve consists of three flaps, but with congenital malformations there can be two and even one leaf. Normally, they open toward the aorta.
At CA, the sash is interconnected due to inflammatory or destructive processes.This leads to a narrowing of the lumen through which blood starts to move from the left ventricle to the aorta under high pressure.
Degrees of gravity of aortic stenosis:
- Lightweight - narrowing not less than 20 mm.
- Moderate - the narrowing is within 10-20 mm
- Expressed - the aperture in the aorta is defined less than 10 mm.
Severe aortic stenosis rarely occurs in infancy, the frequency of occurrence of the defect among live newborns is 0.33%, which is mostly marked by a single-leaf or double-leaf valve.
Pathogenesis of CA
When aortic valve is affected and its stenosis develops, there is resistance to systolic ejection. This obstruction of the outflow of blood leads to an increase in systolic pressure in the left ventricle (LV). As a compensatory mechanism for normalization of the state, the thickness of the walls of the LV increases due to the parallel replication of sarcomers causing concentric hypertrophy. At this stage, the camera does not expand, and the ventricle function is retained.
With prolonged CA development, the ultimate diastolic LV pressure increases, which causes an appropriate increase in pressure in the small arteries of the lungs and a decrease in cardiac output due to diastolic dysfunction. The abnormality of the heart muscle (systolic function) may also decrease, which further contributes to a reduction in cardiac output. Ultimately, heart failure develops.
In many patients with aortic stenosis, the systolic function of the LV is preserved, and cardiac output is not disturbed during many years of life, although with this the systolic pressure of LV can be increased. Despite the fact that cardiac output is normal in a state of rest, it often goes inadequately during exercise, which can lead to the appearance of symptoms on a background of physical activity.
A little statistics on aortic stenosis:
- Aortic sclerosis (calcification of the aortic valve without any obstacles to blood flow, considered as a precursor of calcified degenerative aortic stenosis) increases the incidence of SA with age and is determined in 29% of people over 65 and in 37% of those over 75 years of age.
- Among the elderly, the prevalence of aortic stenosis is between 2% and 9%.
- Degenerative calcined CA is commonly seen in people over 75 and most commonly found in men.
Reasons
Aortic stenosis is congenital and acquired. In each case, the specific causes of the disease are considered.
Congenital aortic valve stenosis
Congenital mononuclear, biconvex, tricuspid or even four-winged valves often contribute to the development of CA. In newborns and children younger than 1 year, a single-valve valve can cause serious contraction. It is the most common anomaly in newborns with a fatal valve stenosis of the aorta. In patients under the age of 15 years, single-valvular valves are most commonly encountered in symptomatic CA.
In adults with symptoms of congenital CA, the problem is usually a double-leaf valve. Such violations do not cause a significant narrowing of the aortic opening in childhood. The modified design of the bifurcated aortic valve provokes the formation of a turbulent flow with a continuous injury of the valves. Ultimately, this leads to their fibrosis, increased stiffness and calcification, and this is a direct path to narrowing the aortic opening in adult life.
The Tzemos study, in which 642 adults with double-wing aortic valves participated, showed that during a follow-up with an average duration of 9 years, the survival rate was not lower than that of the general population. Nevertheless, young people with a biconvex aortic valve had a high risk of surgical intervention due to the reconstruction of the aortic valve. [1 - Ground N; Therrien J; Yip J; Thanassoulis G; Tremblay S; Jamorski MT; Webb GD; Siu SC. Outcomes in adults with bicuspid aortic valves. JAMA 2008; 300 (11): 1317-25]
Congenital anomalies in the form of a tricuspid aortic valve with non-uniform folds ("functionally biconvex" valves) can also cause a turbulent flow leading to fibrosis and ultimately to calcification and stenosis.
Clinical manifestations of congenital aortic stenosis in adults usually occur after the fourth decade of life.
Acquired aortic stenosis
The main causes of acquired aortic stenosis are:
- Degenerative calcification
- Less commonly, rheumatic heart disease.
Degenerative calcification of aortic stenosis (also called senile calcified aortic stenosis) is a progressive calcification of the valve valves, resulting in limited opening during systole.
The risk factors for degenerative calcification of aortic stenosis include:
- old age;
- hypertension;
- hypercholesterolemia;
- diabetes mellitus;
- smoking
In rheumatic stenosis of the aorta, the main process consists of progressive fibrosis of the valve valves with varying degrees of fusion, often with retraction of the edges of the sash and, in some cases, calcification. As a consequence, the rheumatic valve stops the normal passage of blood into the aortic mouth.
Other rare causes of aortic stenosis:
- obstructive vegetation;
- hypercholesterolemia of the homozygous type II;
- Paget's disease;
- Fabry's disease;
- ocheronosis;
- irradiation
It is worth noting that, although differentiation often occurs between tricuspid and bifurcated aortic stenosis, it is often difficult to determine the number of aortic valve flaps. In addition, surgical and pathoanatomical studies confirmed the frequent discrepancy with previously proposed assumptions.
Clinic
Symptoms of aortic stenosis usually develop gradually after an asymptomatic latent period, often lasting 10-20 years.
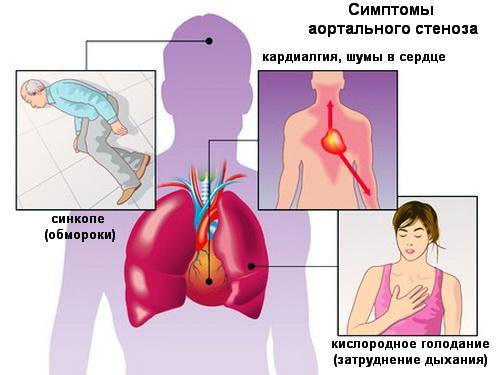
The classic triad of symptoms in patients with aortic stenosis is as follows:
- Pain in the chest: pass through the type of stenocardial pain and usually increase with stress and relax during rest.
- Heart failure: The symptoms of CH include paroxysmal night breath, orthopnea, dyspnea during exercise, and in severe cases, resting.
- Fatigue: often occurs when a load occurs when systemic vasodilatation in the presence of a fixed volume of direct shock leads to a decrease in arterial systolic pressure
Systolic hypertension can be combined with aortic stenosis. However, systolic blood pressure is higher than 200 mm Hg. Art. rarely seen in patients with critical CA.
During physiological examination, the following symptoms of aortic stenosis are determined:
- Pulsus alternans (alternating pulse): may occur in the presence of systolic dysfunction of the left ventricle
- Hyperdynamic left ventricle: suggests the presence of concomitant aortic regurgitation or mitral regurgitation
- Systolic noise: in the classical course of aortic stenosis begins shortly after the first heart sound; the intensity increases to the side of the average size, and ends immediately before the second heart sound
Diagnostics
To assess the general condition of the patient, it is determined:
- Electrolyte in serum
- Heart biomarkers
- General blood test
- Natriuretic peptide of the B-type
From the instrumental methods of diagnostics apply:
- Electrocardiography: A standard ECG can show the progression of aortic stenosis
- Chest X-ray: Changes in heart size are visible in the pictures
- Echocardiography: two-dimensional and Doppler is performed
- Cardiac catheterization: Can be used if the clinical data do not match the results of the echocardiography
- Angiography: an invasive method by which vessels are contrasted
- Radionuclide Ventriculography: Can provide information about LV function
- Stress Test: Contraindicated in symptomatic patients with severe aortic stenosis
Treatment
The only radical treatment of aortic stenosis in adults is the replacement of the aortic valve (surgical or percutaneous). Babies, children and adolescents with double-valves can conduct balloon or surgical valvotomy.
Ambulance
A patient suffering from decompensated heart failure should be delivered as soon as possible to a hospital where he or she can be monitored for pulmonary and cardiac activity. Also, the medical staff will be given intravenous access, through which, if necessary and tolerability will be introduced loop diuretics, nitrates, morphine.
Pharmacological therapy
Drugs used in the treatment of patients with aortic stenosis include the following:
- Digitalitis, diuretics and angiotensin converting enzyme inhibitors (ACEs) are used cautiously in patients with pulmonary obstruction.
- Vasodilators - Can be used for heart failure and hypertension, but they can be used with extreme caution and only by the appointment of a doctor.
Digoxin, diuretics, ACE inhibitors or angiotensin receptor blockers are recommended by the European Society of Cardiology (ESC) / European Association of Cardiac Thoracic Surgery (EACTS) for patients with symptoms of heart failure that can not be surgically treated or transcatheter aortic implantation
Replacement of aortic valve
According to the recommendations of the American College of Cardiology (ACC) / American Cardiology Association (AHA), replacement of the aortic valve can be done in the following cases:
- Significant symptoms are determined due to severe aortic stenosis
- There is asymptomatic, severe aortic stenosis, which has developed due to coronary artery bypass graft surgery
- There is asymptomatic, severe form of aortic stenosis, with the patient having previously undergone an operation on the aorta or other valves of the heart
- On the background of asymptomatic, severe aortic stenosis, systolic LV dysfunction is determined (ejection fraction 0.50)
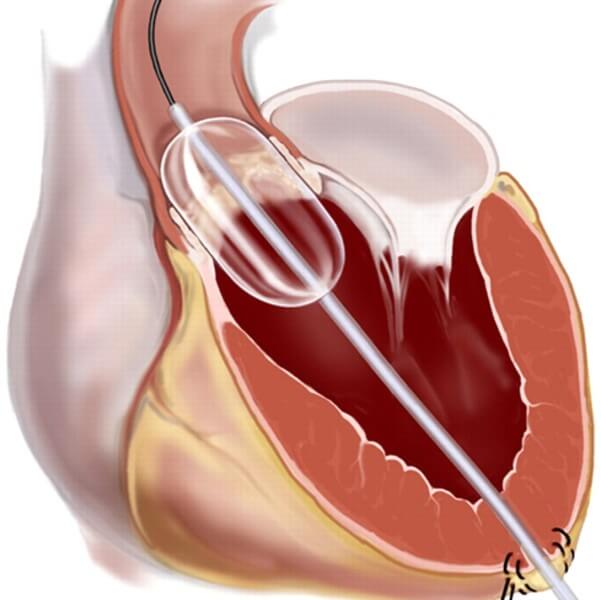
Percutaneous balloon valvuloplasty
This minimally invasive method is used as a palliative measure for the treatment of adult patients in critical condition, which can not undergo a standard surgical operation. In other cases, it is used to temporarily improve the condition of the patient preparing to replace the aortic valve.
Forecast
Asymptomatic patients, even with critical aortic stenosis, provide an excellent survival prognosis with febrile survival rates of less than 1% per year, with only 4% of sudden cardiac deaths in severe aortic stenosis associated with an asymptomatic course of the disease.
Among patients with symptomatic diseases and moderate to severe aortic stenosis, mortality from the onset of symptoms is approximately 25% in the first year and 50% in two years. ore than 50% of deaths are sudden.
Patients with untreated aortic valve stenosis have a poor prognosis when symptoms appear.
Although CA has a tendency to develop more rapidly against degenerative calcining of the aortic valve than with congenital or rheumatic disease, it is impossible to accurately predict the progression rate in individual patients.
Catheterization and echocardiographic studies show that, on average, the area of the valves decreases by 0.1-0.3 square.cm per year;with the systolic pressure gradient through the valve can increase by 10-15 mm Hg.Art.per year.
Rapid progression of CA is observed in elderly patients with coronary artery disease and chronic renal failure.
Video: Live It's great! Aortic stenosis