

Aneurysm
Author Ольга Кияница
2018-03-05
Aneurysm (A.) - is a limited, blood-filled mesh-like convex formed from the wall of the blood vessel. Aneurysms are the result of a weakening of the vascular wall and can be defined as an hereditary condition, and acquired illness. In complicated cases, they are the focus of the formation of thrombosis (thrombosis) and embolization.
Aortic aneurysms resulted in approximately 152,000 deaths in 2013 compared with 100,000 in 1990, as indicated in GBD 2013 Mortality and Causes of Death, Collaborators (December 17, 2014).
As the size of the aneurysm increases, the risk of rupture increases, leading to a hemorrhage. A. can be formed in any blood vessel, but the greatest mortality is observed in the development of aneurysm in the brain, aneurysm of the aorta, aneurysms of the thoracic aorta and aneurysms of the abdominal aorta. A. can occur in the heart after a heart attack, which requires immediate medical intervention.
Video of aneurysm: "bomb of delayed action"
Classification
Aneurysms are divided according to the morphological features, location and mechanisms of development.
Classification of aneurysm by location:
- Arterial and venous, though more common arterial species.
- Cardiac, including coronary aneurysms, ventricular aneurysms, Valsalve sinus aneurysm and aneurysms that have arisen after cardiac surgery.
- Cerebrovascular, including cerebral aneurysms, berry aneurysms and Sharko-Bushard aneurysms.
- Lower limb aneurysms, including popliteal arteries.
- Renal aneurysms, including renal artery aneurysms.
- Capillary aneurysms.
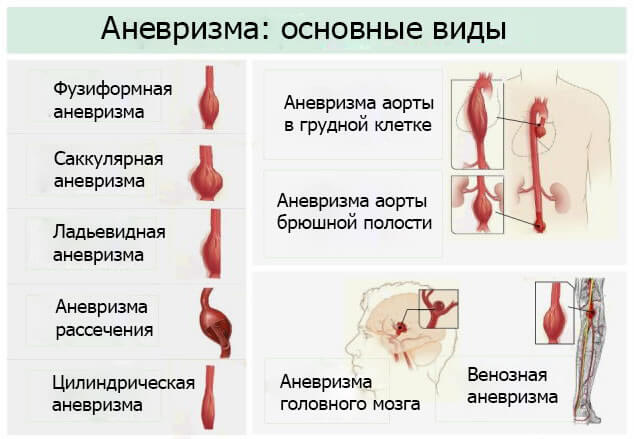
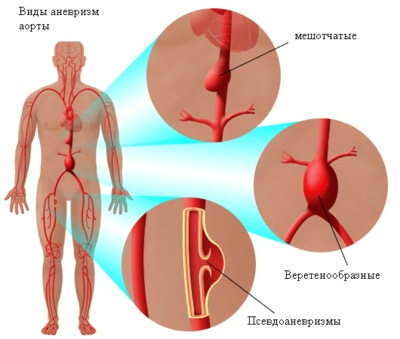
In morphology, which takes into account the size and macroscopic form, aneurysms are divided into:
Succulent aneurysms that are spherical. When they are formed, only part of the vessel wall is involved in the pathological process. Their sizes vary from 5 to 20 cm in diameter, while often filling, partly or completely, with a thrombus.
Fusiform aneurysms , known as spindle-shaped. They differ both in their diameter, and in length. The diameter of such aneurysms can reach 20 cm. They are often formed on the ascending and transverse arch of the aorta, abdominal aorta, and rarely in the pelvic arteries.
Also distinguished by rowing aneurysms, cylindrical and aneurysms of the dissection.
The form of aneurysm is not strictly specific, therefore pathological education can occur in various diseases.
.
According to the mechanism of development of aneurysm there are two types:
True - include all three layers of the artery wall (intima, middle part and adventitia). True aneurysms are atherosclerotic, syphilitic and congenital A., as well as A. ventricles, which develop as a result of transmural myocardial infarctions (aneurysms affecting all layers of the weakened heart wall are also considered true).
False, or pseudoaneurysms - is the blood that has escaped from the artery or vein, which was limited to tissue located near the vessel. In the future, such an education either turns into a thrombus, or breaks the surrounding tissues.
Reasons
Aneurysms are formed under the influence of several interacting causes.
The main etiological factors include:
- Atherosclerosis. With the development of this disease, the walls of the blood vessels are weakened. Under the action of blood flowing through the vessel, further degeneration of the vascular wall occurs.
- Hypertonic disease. It often exacerbates the formation of aneurysms and accelerates its expansion. Moreover, the more A extends, the stronger the voltage on the vascular wall increases. Blood pressure in the expanding aneurysm can also damage the blood vessels supplying the artery, which further weakens the wall of the vessel. Without treatment, these aneurysms will eventually develop and rupture.
- Infectious diseases. They lead to the development of mycotic aneurysms, which arises as a result of the infectious process affecting the arterial wall. A person with mycotic aneurysm has a bacterial infection in the artery wall, which leads to the formation of aneurysms. Such formations most often affect the arteries in the region of the abdomen, thigh, neck and hands. In severe cases, it can lead to sepsis or lethal bleeding when rupture of the aneurysm. Less than 3% of the aneurysms of the abdominal aorta are mycotic aneurysms.
- Syphilis During the third stage of the disease, aneurysm of the aorta can be formed, which is due to the loss of the tone of the adventitia of the vessel
- Copper deficiency. A small amount of aneurysm is caused by copper deficiency, which leads to a decrease in the activity of the lysiloxidase enzyme, which affects elastin, a key component of the walls of the vessels. Copper deficiency leads to thinning of the vessel wall and, thus, leads to the death of patients with a similar pathology.
It is worth noting that pseudoaneurysms are formed due to an injury that pierces the artery (for example, knife and bullet wounds).It can also occur on the background of percutaneous surgical interventions such as coronary angiography or intraarterial injection.
An earlier formed aneurysm may break down and this happens for the following reasons:
- Sharp increase in blood pressure (hypertensive crisis).
- Excessive physical stress.
- Pregnancy and childbirth.
- Strong stress.
Risk factors
- Diabetes
- Obesity
- Hypertension
- Smoking
- Alcoholism
- High cholesterol
- Copper deficiency
- Old age
- Tertiary syphilis infection.
Infectious diseases contributing to the development of aneurysms:
- Progression syphilis, which leads to syphilitic aorta and aortic aneurysm.
- Tuberculosis causing Rasmussen's aneurysm.
- Brain infections that stimulate the development of infectious intracranial aneurysms.
A little aneurysm is associated with genetic factors. For example, aneurysms of the circulatory artery artery associated with autosomal dominant polycystic kidney disease are diagnosed. Family aneurysms of the thoracic aorta are also determined.
Species
The most common aneurysms, such as A. arteries of the brain, A. aorta, A. heart, will be considered.
Aneurysm of the arteries of the brain
It occurs quite often, as a large part of the population suffers from hypertension, which is a direct threat to the immediate development of A. With its formation in the arteries of the brain, a local extension is formed. In severe cases, A. is complicated by hemorrhage, which leads the patient to death. With the breakdown of A. artery of the brain, only half of the patients remain alive and that most of them become disabled.
A. Brain arteries are difficult to diagnose, since they are often perceived as a tumor.Less than a quarter of patients experience migraine-like headaches during her development.
Cerebral aneurysms, also known as intracranial or cerebral aneurysms, are most commonly encountered in the anterior cerebellar artery, which is part of the Willis circle. This can lead to serious injuries leading to death. The following most common places for the onset of aneurysm of the brain are the internal carotid artery.
Video Aneurysm of the vessels of the brain
Aneurysm of the aorta
A dangerous condition that can lead the patient to death very quickly. Each year, such a diagnosis as the aneurysm of the aorta, put more than 50 thousand.Man Also, in 7% of the dead from another cause A. aorta is determined.
A. aorta manifests itself in rare cases and most often in later stages. In this case, patients feel painful pressure in various parts of the body.
Aorta is the largest vessel in the human body, which is divided into various parts. In the development of A. indicate the department in which it was formed. In particular, the A. thoracic division of the aorta, abdominal, etc., is distinguished. The course of A. aorta can be different. For example, with A. abdominal pain, pain is often felt, which is more pronounced in thin patients or when pushing the roots of the spinal cord.
Heart aneurysm
Often arises after myocardial infarction, when the wall of the left ventricle stretches or weakens. A similar occurrence occurs in 35% of cases immediately after a heart attack, although it happens that it takes several months after a heart attack and only then aneurysm is determined.
Among patients with MI, the incidence of aortic aneurysms is 5-20%.
Any kind of aneurysm presents a danger to the health and even the life of the patient, therefore, when it is detected, all measures for the provision of medical care should be taken.
Clinic
Aneurysm is practically not manifested if it is small in size or does not overbalance any nerve fibers. If the aneurysm ruptures, then the following clinical picture develops:
- Headache (mainly observed during cerebral aneurysm). It is often presented to the patient as a sudden blow, quite sharp and pulsating in the area of the nape. In some cases, pain becomes burning and burning.
- Nausea, which is accompanied by multiple vomiting.
- Increased body temperature.
- Bad perception of light and noise.
- Psychomotor agitation.
The most pronounced clinic for cerebral aneurysm, because when it breaks, important motor-sensitive centers of the brain are damaged. With this pathology, the following symptoms are observed:
- Fatigue and weakness
- Violation of perception
- Equilibrium disorder
- Problems with speech
- Double vision
The ligament of the caudal muscles is an important diagnostic symptom manifested by the hypertonicity of the cervical muscles, due to which the patient can not bring the head to the chest in the lying position. Appears when lesions of the meningeal membranes, therefore together with other indications, is the meningeal syndrome.
In severe cases, the patient may experience convulsive conditions and even loss of consciousness, up to the coma.
Diagnostics
Definition of complaints and physical examination of a patient (including auscultation, pressure measurement and neurological examination) is necessarily supplemented by instrumental research methods.
First of all angiography is conducted - it is a "gold standard" in determining the aneurysm of any localization. If necessary, this diagnostic method is combined with magnetic resonance imaging and computer tomography. If problems arise with the diagnosis, then other methods of research are used:
- The ultrasound of the abdominal aorta and other parts of the body.
- Positron emission tomography (allows to determine weakened or strengthened blood circulation).
- Lumbar puncture (the composition of the cerebrospinal fluid is estimated, in which blood will be determined by breaking the cerebral aneurysm).
Treatment
Medical aortic aneurysm therapy includes strict control of blood pressure. This does not apply to the aneurysm of the aorta as such, but control of hypertension under conditions of maintaining blood pressure in the permissible range may reduce the rate of expansion of the aneurysm.
Medical treatment for patients with small aneurysms suggests:
- cessation of smoking;
- blood pressure control;
- the use of statins and sometimes beta-blockers;
- regular conduct of an ultrasound (that is, every six or 12 months) to monitor the size of the aneurysm.
Surgical treatment
Fast-growing aneurysm should be removed in normal circumstances as soon as possible, as there is a high risk of rupture. Slowly expanding aneurysms of the aorta can be accompanied by routine diagnostic testing (ie CT or ultrasound examination).
For abdominal aneurysms, current guidelines for treating aneurysm of the abdominal aorta involve a planned surgical operation, especially if the diameter of the aneurysm exceeds 5 cm. However, recently obtained data on patients aged 60-76 years indicate that in this age a medical treatment of abdominal aneurysm should be performed with a diameter of less than 5.5 cm.
The decision to restore aortic aneurysm is based on the balance between the risk of breaking aneurysms without treatment and the risks of the treatment itself. For example, a small aneurysm in an elderly patient with severe cardiovascular disease is not desirable surgically removed. The probability of a small aneurysm rupture is less than the risk of cardiac complications from the on-line procedure.
The operation is accompanied by the following risks:
- There is a risk of problems occurring during and immediately after the procedure itself ("periprocedural" complications).
- The effectiveness of the procedure must be taken into account, namely, whether this operation effectively protects the patient from the breakdown of aneurysm in the long run and whether the procedure is so robust that repetitions are not necessary.
These problems are important and should be taken into account when choosing between different treatment options. Less invasive procedures (eg, endovascular occlusion of the aneurysm) may be associated with fewer short-term risks for the patient (less perioperative complications), but secondary procedures may be required for long-term observation.
The final treatment of the aneurysm of any localization is accomplished by performing an open operation or endovascular occlusion. Determining the volume of surgical intervention is a complex decision that is taken on a case-by-case basis.
The risk of aneurysm rupture is correlated with procedural risk. The diameter of the aneurysm, its rate of growth, the presence or absence of Marfan syndrome, Ehlers-Danlos syndrome, or similar connective tissue disorders and other concomitant diseases are important factors in general treatment.
Forecast and prevention
In most cases, the aneurysm should be surgically removed because of the high risk of fracture. Only small aneurysms can remain under continuous observation, especially if the patient has severe concomitant illnesses.
With the exception of risk factors or minimization of their effects, the prognosis for relatively small aneurysms is relatively favorable.
After the breakdown of the aneurysm, the degree of consequences affected by it is determined:
- age of the patient;
- localization of aneurysm;
- the severity of bleeding;
- the speed of medical care.
In the case of rendering of fast medical aid at break A., as well as carrying out an effective operation, patients are rehabilitated with almost no consequences in the period from a few weeks to a couple of months.
У меня аневризм почечной артерии правой,куда только не обращал ась не кто толком не объясняют,просто жду,когда помру,амне 61 лет
Галина, если аневризма небольшая, тогда больного просто наблюдают. Если размеры аневризмы увеличиваются или появляются новые симптомы, проводят хирургическое вмешательство, чаще всего эндоскопическое иссечение аневризмы. Болезнь опасна своими осложнениями, поэтому лучше даже при небольших размерах образования не медлить с оперативным лечением.